


The pediatric population is known for their strong compensatory mechanisms, even in the face of considerable illness and injury. Hypotension doesn’t typically occur until pediatric patients have lost a considerable amount of their blood volume; at that point, emergent fluid resuscitation is key to preventing further clinical deterioration including organ damage and cardiovascular collapse. Each additional hour that a child remains in shock leads to a greater than two-fold increase in their odds of death.1 For children in decompensated shock (hypotension with delayed capillary refill), mortality is over 30%.1
Rapid fluid administration is a key component of early shock reversal. For hypovolemic shock, the most common form of shock in pediatric patients, 2016 Pediatric Advanced Life Support (PALS) guidelines recommend rapid fluid boluses of 20 ml/kg of isotonic crystalloid by IV or IO, reassessing perfusion and cardiorespiratory status carefully during and between each bolus.2 Recently there has been a lot of discussion around the guidelines and methods for fluid resuscitation. Traditional methods of rapid fluid administration include rapid infuser machines, pressure bags, and the “push-pull” method. In order to explore the fluid resuscitation related perceptions and practices of pediatric nurses we conducted a survey at a recent pediatric nursing conference. This blog will summarize the key findings of the survey, pointing out challenges, knowledge gaps and opportunities for improvement regarding pediatric fluid resuscitation.
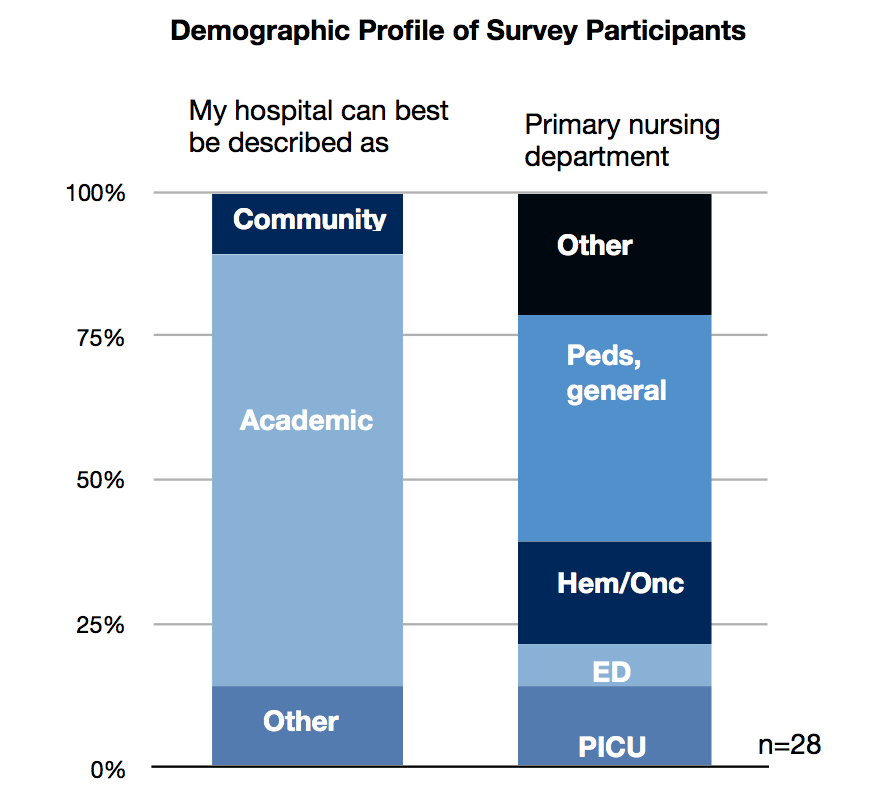
The survey was conducted at the 2019 annual SPN (Society of Pediatric Nursing) conference held in Washington D.C. Twenty eight (28) pediatric critical care or emergency medicine nurses were surveyed. The key themes explored in the survey included: (1) perceived role of fluid resuscitation in patients with hypotension or shock, (2) current method(s) for delivery of rapid IV fluids and perceived pros and cons, and (3) the perceived contamination risk related to the push-pull technique.
Role of fluid resuscitation
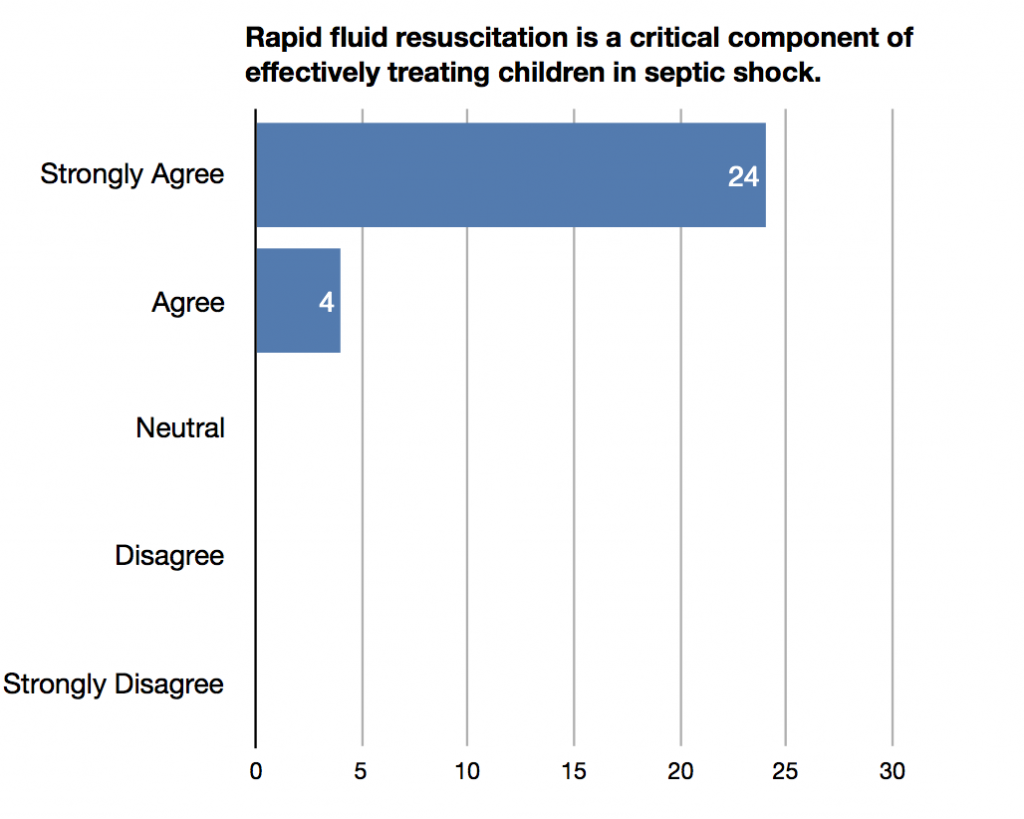
All of the nurses surveyed (100%) “strongly agreed” or “agreed” that fluid resuscitation is a critical early step for treating children with hypotension and that early reversal of hypotension and shock can help avoid additional interventions. In addition, 93% of the nurses surveyed believe that early reversal of shock and hypotension can help avoid excess fluids for that patient throughout the continuum of care.
Current Methods
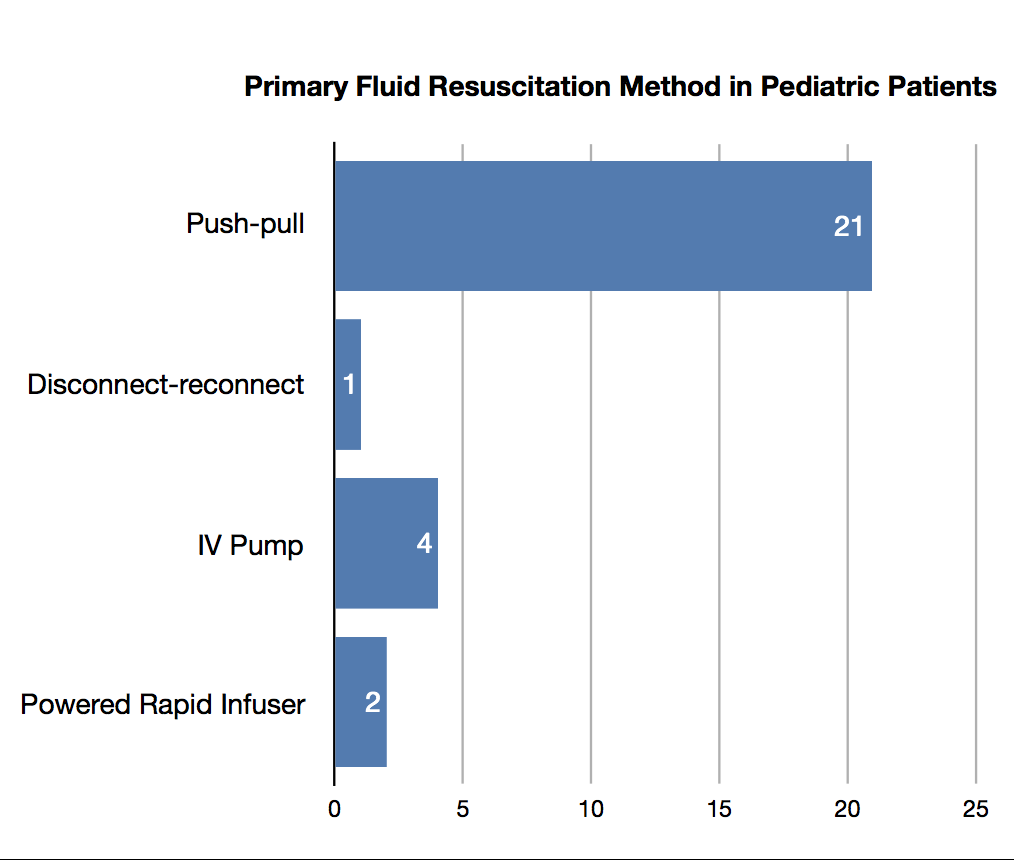
Most (82%) of the survey participants reported that their hospital’s protocol for pediatric fluid resuscitation included guidelines for delivering 20ml/kg boluses, consistent with guidelines published by national organizations such as the American College of Critical Care Medicine (ACCM) and the American Heart Association (AHA). Four different methods, push-pull, disconnect-reconnect, IV pump and powered rapid infuser, were referenced as the primary method of fluid resuscitation in pediatric patients with shock or hypotension.
None (0%) of survey participants were satisfied with the current methods of rapid fluid delivery. The most commonly reported challenges included (1) difficulty getting the fluids in quickly (cited by 71%), (2) difficulty with complex or slow equipment set-up (cited by 53%) or (3) IV infiltration (cited by 29%) and 100% of the respondents stated that a new fluid bolus device that could reduce complexity and stress in a code situation would be very beneficial. The nurses’ concerns were consistent with prior literature that cites current fluid delivery methods as barriers to achieving target rates and volumes of IV fluids given during fluid resuscitation.3,4
Contamination Risks Associated with Push-Pull Technique
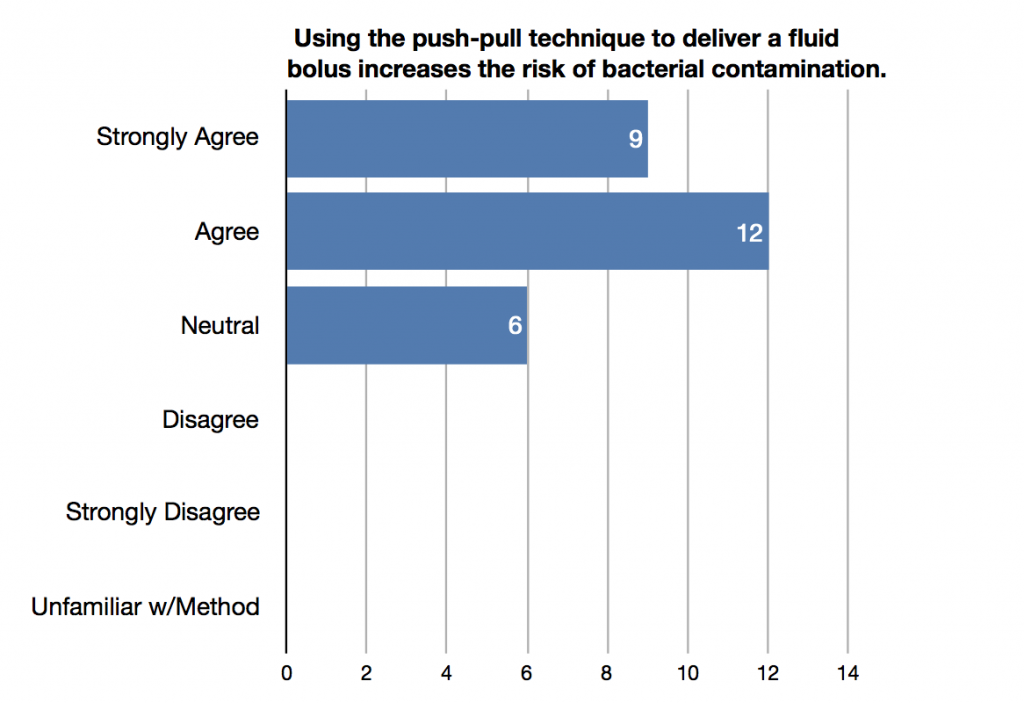
A recent study by Spangler et al.3 compared aseptic technique violations using two different methods for rapid IV fluid delivery in a simulated patient model. The authors reported that the push-pull technique of fluid delivery was associated with multiple aseptic technique violations related to contamination of the syringe barrel. Approximately 75% of the nurses surveyed at the SPN conference “agreed” or “strongly agreed” that the push-pull technique for fluid bolus delivery increases the bacterial contamination risk, and approximately 60% perceived this risk as “high” or “very high.” Since 100% of the nurses surveyed reported that CLABSI reduction is a major priority in their hospital, the possibility of bacterial contamination during the push-pull technique of rapid fluid administration is a major concern.
Summary
Children with hypotension and shock require rapid intravenous fluids to correct hypotension and prevent complications such as organ damage and cardiovascular collapse.4 Although the number of participants in this survey was relatively small, there is very strong agreement on several key points:
- Early, rapid fluid resuscitation is a critical part of treating children with shock or hypotension
- The traditional methods of fluid resuscitation have significant drawbacks and a new faster, easier method would be valuable
- The push-pull technique presents a significant contamination risk
Additional market research could be performed to confirm the results of this survey.
LifeFlow® is a new method for fluid resuscitation that has been used to successfully resuscitate children in shock.5
Interested in learning more about rapid, controlled delivery of a fluid bolus with LifeFlow? Contact us.
- Carcillo JA, Kuch BA, Han YY, et al. (2009). Mortality and functional morbidity after use of PALS/APLS by community physicians. Pediatrics.124:500–508. doi:10.1542/peds.2008-1967.
- American Heart Association (2016). Pediatric Advanced Life Support Provider Manual.
- Spangler, H., Piehl, M., Lane, A., Robertson, G. (2019). Improving aseptic technique during the treatment of pediatric septic shock: A comparison of 2 rapid fluid delivery methods. Journal of Infusion Nursing: 42(1); p 23–28. doi: 10.1097/NAN.0000000000000307.
- Paul, R., Neuman, M. I., Monuteaux, M. C., & Melendez, E. (2012). Adherence to PALS sepsis guidelines and hospital length of stay. Pediatrics, 130(2), e273-e280.
- Piehl, M., Smith-Ramsey, C., Teeter, W.A. (2019). Improving fluid resuscitation in pediatric shock with LifeFlow: a retrospective case series and review of the literature. Open Access Emergency Medicine. Doi: https://doi.org/10.2147/OAEM.S188110.